
- Curettage of the periodontal pocket
- Gingivectomy
- Air flow
- Periodontal surgery
Curettage of the periodontal pocket
The soft wall of the periodontal pocket forms part of the free gingiva that extends from the edge of the gingiva apical to the bottom of the periodontal pocket. This part of the gingiva is on the inside (which is turned towards the tooth) covered by the epithelium of the periodontal pocket. This epithelium of the periodontal pocket actually represents former epithelial gingival sulcus, which is pathologically modified in that it is degenerate, with the appearance of ulcerous-necrosis lesions on it. This pathologically modified epithelium is necessary to remove.
The procedure by which all these pathologically altered tissues are removed from is named curettage, and therefore the entire therapeutic procedure has received the name of a periodontal pocket curettage or a periodontal pocket treatment.
The curettage simultaneously eliminates proliferated epithelial buds and chronic inflamed granulation tissue. When processing the soft wall of the periodontal pocket, it is necessary to remove the remains of the pathologically altered adherent epithelium located at the bottom of the parodontal pocket. By removing granular tissue from the surface of the soft wall of the periodontal pocket, it is easier to access the bottom of the periodontal pocket and the hard wall and its easier processing. Removal of granulation tissue reduces bleeding, which creates the conditions for successful treatment of the hard wall of the periodontal pocket.

Gingivectomy
Gingivectomy is a surgical procedure for the removal of periodontal pockets. The term “gingivectomy” refers to the cutting of the gingiva, and is derived from the word “gingiva” and “ectome” (“sections”). During gingivactomy, the gingiva is not removed completely, but only part of it that forms the soft wall of the periodontal pocket. Gingivectomy can also correct some irregularities in terms of gingival forms. Applied exclu- tingivectomy is indicated and relatively good results are achieved in cases of: – deep supraxtension periodontal pockets; – periodontal pockets whose soft wall is fibrous, ie firm and rigid, due to the proliferation of connective tissue. In the case of such pockets, treatment of periodontal pockets will not give good therapeutic results, as the edge of the gingiva will remain at the same level as before the therapy; – Suprared periodontal pockets whose soft wall is slim, so that during their processing it will be torn or torn; – gingival pockets caused by hyperplasia of the gingiva; – crater in interdental papillomas produced after ulceronecrosal gingivitis; – short clinical crowns of the tooth where after the gingivactomy there is an extension of the clinical toothbrush that is often necessary for prosthetic reasons – periodontal abscesses in shallow periodontal pockets of the supra-type type. This intervention refers to chronic periodontal abscesses, as well as those of acute flow, all only after calming acute symptoms.
Gingivectomy will not give good therapeutic results and is not indicated in cases of: – infrared periodontal pockets; – periodontal pockets whose bottom is near the musculoskeletal line or is more apical than it; – if gingiva is caught; – if the cut in gingivactomy should be provided in the immediate vicinity of the attachment of the frenulum or plaque. Gingivectomy is performed under the usual anesthesia where the anesthetic is accelerated into the interdental papillae, from the vestibular and the oral. Then the depth of the periodontal pockets is determined and marked. This is done by special instruments (“markers”). These are instruments with one arm thin and spike, similar to the probes, while at the top of the second arm there is a tooth at an angle of 90 degrees relative to the arm of the instrument. The right marker mark is inserted into the periodontal pocket to its bottom and then the instrument is closed so that the tooth pierces the gingiva (the soft wall of the periodontal pocket). After removing the instrument, the blood point remains on the surface of the gingiva, indicating the depth of the periodontal pocket. Determining and marking the depth of the periodontal pocket can also be carried out by a probe: it first measures the depth of the pocket, which is then transferred from the outside to the gingiva, and then the level of the bottom of the periodontal pocket is marked with the tip of the instrument. This marking is performed systematically from one end to the other end of the operative field from the vestibular and oral sides.
Air flow
Removal of soft deposits and pigmentation of teeth in modern dentistry is done today by the Air-Flow® system, and the procedure is called tooth sandblasting. Our treatment with this method reliably removes the stains from wine, cigarettes, coffee or tea from your teeth, from a place where traditional ultrasound removal of toothpaste has failed.
Sandblasting is not and can not be seen as a tooth whitening treatment, but the effect achieved after treatment gives your teeth a single shade of white teeth, smooth and noticeably shiny. This, practically, detox therapy of the whole lip syringe is carried out by a special apparatus designed to expel aerosols and water to the surface and between each tooth under strong pressure.
The treatment is completely painless for the patient and lasts about 20 minutes on average. It is recommended as part of teeth whitening preparation and part of your everyday healthy and brilliant smile.
Periodontal surgery
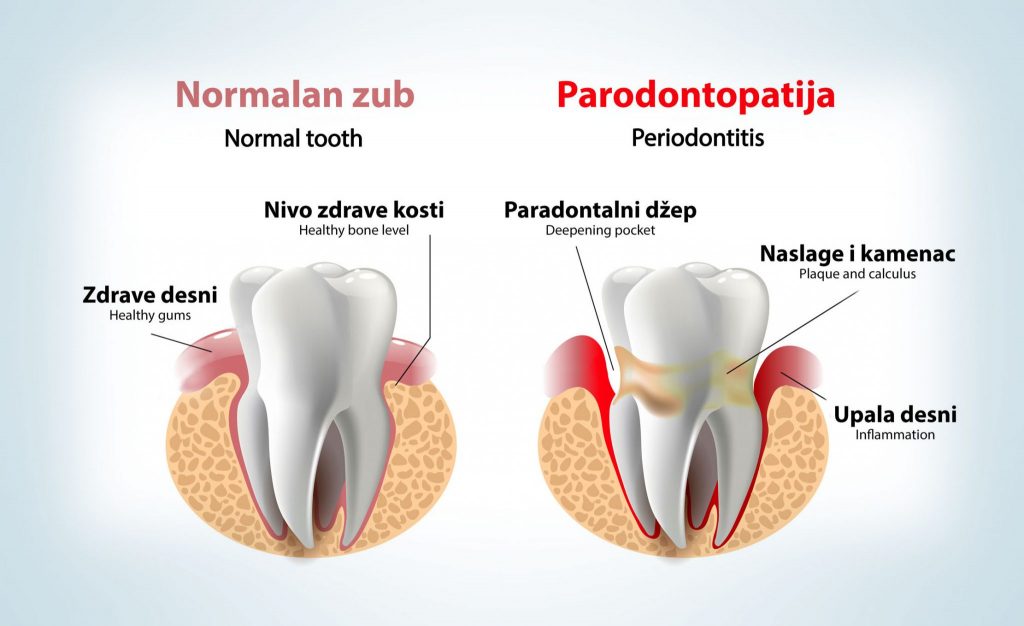
Parodontopathy is a very widespread chronic disease during which there is a gradual withdrawal of the gums, loss of bone mass and the formation of periodontal pockets, and in the advanced stage, the final loss of teeth also occurs.
MAKE AN APPOINTMENT
Fill out the contact form and book an appointment. We will be happy to answer all your questions!







